Medical records not only provide pertinent information about your patients, but they can also protect you against false claims of negligence. Without proper documentation, the veterinarian runs the risk of being unable to provide proof of appropriate care in the event of a malpractice claim or license complaint. Even exemplary advice and patient care is difficult to prove without documentation. If a client files a board complaint or makes a claim of negligence, your medical records are your most valuable asset to defend your standard of care.
When it comes down to an allegation of malpractice, many attorneys will argue that “if it isn’t documented in the medical record, it didn’t happen”. Courts and state licensing agencies expect accurate documentation and charting from veterinary professionals. Inadequate record keeping can compromise the veterinarian’s defense during trial or board review. Although licensing agencies receive relatively few client complaints on record keeping, the veterinarian’s medical records often become the central issue when the complaint is reviewed by the state veterinary board, even when the initial complaint is dismissed.
Good Record Keeping is…
- Required by state veterinary boards and practice acts
- Evidence to support your standard of care
- Easy to read and follow
- Helpful to resolve client disputes
- Key to your defense in a malpractice claim or board complaint
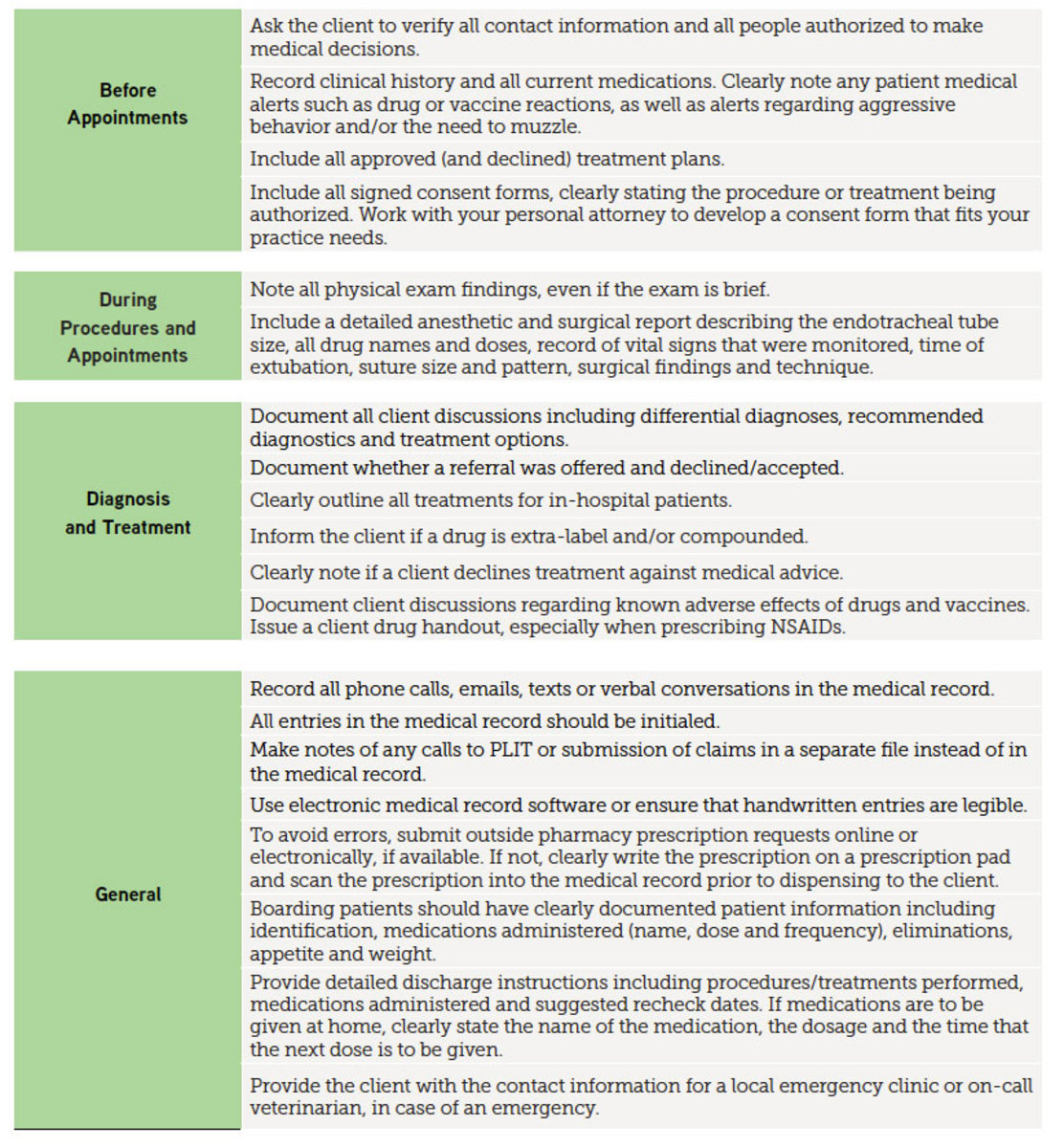
Recordkeeping Best Practices
The chart below provides PLIT’s recommendations for thorough recordkeeping across the spectrum of patient and client interactions.
Documentation Errors to Avoid
- Illegible handwritten entries. This makes it difficult and confusing for another veterinarian or technician to follow your treatment plan, increasing the risk of medical errors.
- Including inappropriate entries in the medical record. Negative comments about the client or animal as well as offensive language should not be part of the medical record. Only enter information pertinent to the medical care of the patient into the medical record.
- Failing to document patient status and medications administered to boarded patients.
- Failing to keep a detailed anesthesia report, verifying that the patient was adequately monitored while under anesthesia and during post-operative recovery.
- Failing to write a detailed surgical report.
- Failing to provide discharge instructions in writing.
- Failing to confirm that consent forms have been signed by the client.



![[Aggregator] Downloaded image for imported item #19769](https://s3.amazonaws.com/wp-s3-equimanagement.com/wp-content/uploads/2026/05/31141823/EDCC-Unbranded-11-scaled-1-768x512.jpeg)