During a Burst session at the 2025 American Association of Equine Practitioners, Jaret Pullen, DVM, APF-I, of JP Hoofworks, walked attendees through the steps he takes when treating solar punctures. “There are very few podiatry emergencies that ‘Can’t wait till morning,’” he said. “This is one of those that cannot wait until morning.”
When you first get the call from the client, make sure they know to leave the foreign object in place. Have the owner implement temporary hoof protection and relief for the horse while you’re en route. Pullen described one case where the owner affixed a roll of Duct tape to the bottom of the horse’s foot—an effective strategy because it has a giant hole in the middle and can withstand the weight of a horse. Another cut a hole out of the center of a hoof boot.
“Be creative,” he said. “Protect the wound with a wooden donut, foam, Duct roll, anything.”
The Initial Assessment
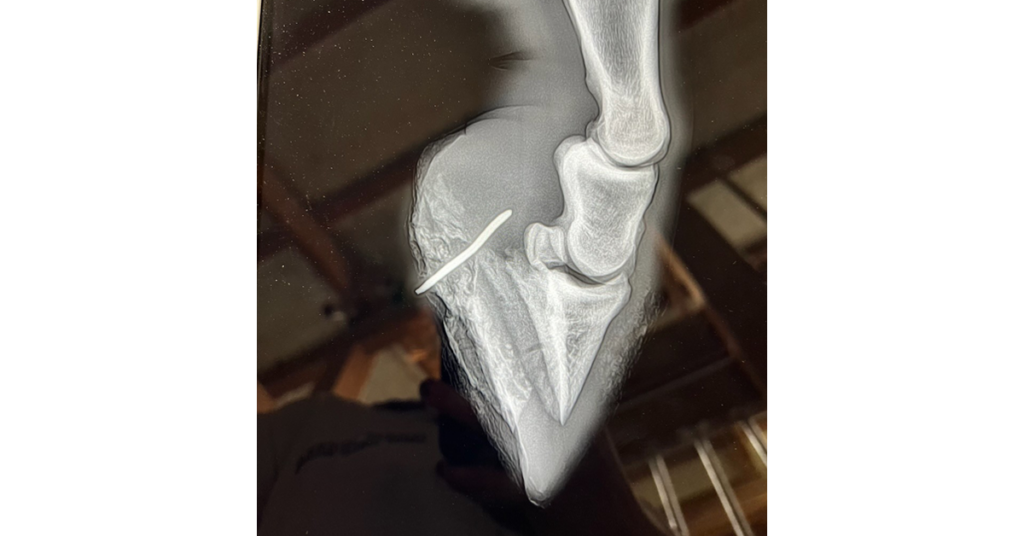
The first step? Identify the extent of the puncture wound and whether it’s near a synovial structure. Pullen said he’s a big proponent of performing stallside CT, which will provide you with every oblique image you need. Otherwise, if the foreign body or nail is still intact, take radiographs.
“Know your anatomy, and know exactly where your synovial structures end,” he advised. “Think about whether you want to do a fistulagram versus an arthrogram or a bursagram—it’s going to depend on where that nail is.”
If the nail is no longer present, determine whether you can see the tract. “The horse’s foot has an amazing ability to make a tract disappear once that foreign body is pulled out,” Pullen noted.
Without a visible tract, make sure you have sharp hoof knives (consider getting autoclave knives that retain their sharp edge) to help you find it. Once you do, there a few methods you can use to explore it. He recommended irrigating the wound using a tool such as a gavage needle, teat canula, or catheter.
“I like to use dilute 1% povidone iodine if there is a question that it’s anywhere near a synovial structure,” said Pullen. “It’s going to be safer than chlorhexidine.”
If you know the wound is nowhere near a synovial structure, you might perform a contrast fistulagram to see where the contrast medium goes. “If not, maybe an arthrogram or a bursagram is going to be more important,” he said. “If you’re already going into the joint, add some amikacin. If you don’t have any contrast, see if you can distend that synovial structure—see if it’ll hold the pressure.”
Lastly, take more radiographs using a sterile flexible blunt probe to determine the wound’s depth.
Mechanical and Surgical Approaches

In preparation for surgery, trim some foot and use a rasp or sandpaper to scuff the hoof wall and remove the soiled layer. Pullen said he applies a shoe with impression material before the procedure, so he can simply add the hospital plate once the surgery is done.
He urged practitioners to take a funnel-shaped surgical approach, in which the distal part of the wound is much wider and tapers down into the lesion, to encourage healing from the inside out. Clean the wound and pack it with antimicrobial gauze, then place the hospital plate with some level of mechanics. Pullen advised applying the plate with one bolt, instead of four, if possible, for client compliance and easier bandage changes.
“With a lot of these, I’ll really increase the palmar angle, especially if (the puncture) is going through the deep digital flexor tendon,” he said. “We want to slack that tendon as best we can for healing and drainage.” You can then lower the palmar angle as healing progresses.
You might also do regional limb perfusions, with or without systemic antibiotics, and perform general wound care like you would with any other lesion.
Don’t Neglect the Other Foot
“Often we can win with the foot with the huge nail sticking out of it, but that horse might still end up 6 feet under due to contralateral limb laminitis,” Pullen reminded attendees.
He recommended taking baseline venograms on the contralateral foot on Day 1, followed by serial venograms to monitor its condition, especially in cases with prolonged non-weight-bearing. Add mechanical support (e.g., NanricUltimates) to the contralateral foot.
“Have that discussion about outcomes and contralateral laminitis with the owner so they know why you’re doing it and what the long-term effects are,” said Pullen.
Related Reading
- Treading Lightly: Managing the Thin-Soled Horse
- Is Colloidal Iron an Effective Hoof Disinfectant?
- Tips and Tricks to Acquiring Great Equine Foot Radiographs
Stay in the know! Sign up for EquiManagement’s FREE weekly newsletters to get the latest equine research, disease alerts, and vet practice updates delivered straight to your inbox.



![[Aggregator] Downloaded image for imported item #19769](https://s3.amazonaws.com/wp-s3-equimanagement.com/wp-content/uploads/2026/05/31141823/EDCC-Unbranded-11-scaled-1-768x512.jpeg)